
Traumatic Brain Injury and Epilepsy
What is traumatic brain injury (TBI)?
TBI is a well-recognized cause of seizures and epilepsy. Traumatic brain injury (TBI) is the result of an external force on the head. TBI can occur as a result of the following:
- The head suddenly and violently hitting an object (falls, car accidents, sports injuries)
- Severe shaking of the head (child abuse)
- An object piercing the skull and entering brain tissue (gunshot wound, military combat)
- Pieces of the skull compressing or penetrating brain tissue (skull fractures)

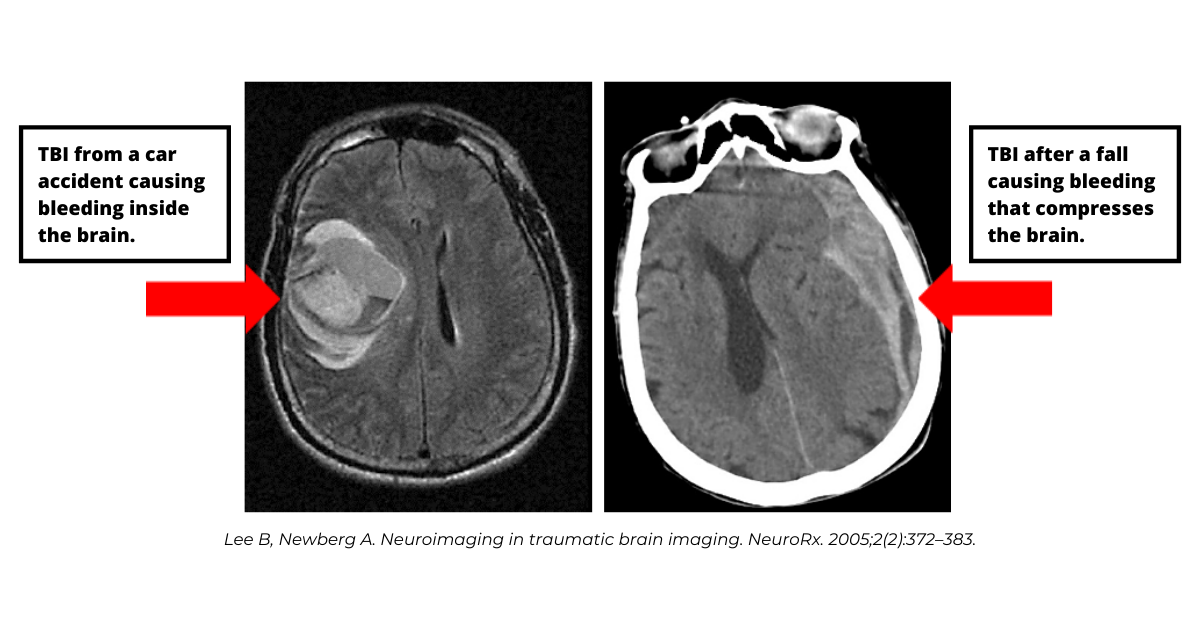
Depending on the type and severity of trauma a person experiences, TBI may cause bruising of the brain (brain contusion), bleeding inside the brain (intracerebral hemorrhage), bleeding between the coverings of the brain and the brain (subdural or subarachnoid hemorrhage), bleeding between the skull and coverings of the brain (epidural hematoma). Even if bleeding occurs outside of the brain it can have an impact on brain tissue by compressing the brain and disrupting normal brain anatomy and function. TBI can also cause mild to severe swelling of the brain (intracerebral edema).
A person who has a TBI needs medical attention as soon as possible. Most often it is not possible to reverse the damage caused to brain tissue by trauma but receiving prompt medical care may make it possible for medical providers to stabilize a person’s brain injury and help to prevent further injury.
How common is TBI?
The Centers for Disease Control and Prevention (CDC) estimated that in 2014 TBIs accounted for approximately 2.87 million emergency room visits, hospitalizations, and deaths in the United States, either as an isolated injury or in combination with other injuries (288,000 hospitalizations, 56,800 deaths). (Centers for Disease Control and Prevention (2019). Surveillance Report of Traumatic Brain Injury-related Emergency Department Visits, Hospitalizations, and Deaths—United States, 2014.).
How are people impacted by TBI?
Traumatic brain injuries can range from mild, to moderate, to severe and as a result the spectrum of impact on any individual can vary. The terms mild, moderate and severe refer to the severity of the trauma not the consequences from the TBI. Mild trauma to the brain may affect brain cell function for hours, days or weeks. More severe brain injuries often have more long-term effects and can result in significant disability or death. A range of both physical cognitive and psychiatric symptoms can be present after a traumatic brain injury. In addition, changes in movement, sensation, vision and hearing are possible and seizures and epilepsy are a relatively frequent complication of TBI. The area of the brain affected by the injury, the extent of the brain injury and the age and general health of a person before the injury will determine how a person is impacted.
What tests are done to assess TBI?
Each person with a traumatic brain injury should undergo medical and neurologic evaluations. The setting of the injury, the severity of the injury, and the neurologic and medical conditions of the person will help to determine the need for further evaluations, including neuropsychologic testing and the immediate versus late treatments offered to a person.
Brain imaging with CT and when available brain MRI studies and electroencephalography (EEG) are routinely used to assess the degree of brain injury after a trauma. Blood work will also be done to identify any toxic, infectious or endogenous cause that may have facilitated the development of the head trauma and identify any blood loss.
A person who has a head injury will also be assessed for injury to the cervical spine (neck) and spinal cord. The mechanism of traumatic injury (blow to the head, jolt or whiplash, penetrating injury, open (skull is open) versus closed (skull intact) head injury is carefully considered in decisions about testing. Severe head trauma with brain injury is often accompanied by other bone or organ injuries and evaluation for other bodily injury may need to be done.
What treatments are used?
The type of treatment a person receives for a TBI will depend on the severity of the brain injury, the symptoms, the clinical exam and test findings. Each person’s individual treatment will be determined by their doctor. For some people with a mild TBI, rest and observation at home may be all that is necessary. For others with moderate to severe TBI, emergency hospitalization, anti-seizure medications, ICU level care, surgery and other life-saving stabilization of injuries and treatments may be necessary.
What do we know about seizures and TBI?
Seizures can occur early (within the first week of the brain injury), or late ( more than a week after brain injury). Seizures which occur early after a traumatic brain injury are felt to be a symptom of the recent injury. Seizures which occur in the late period after TBI are more likely to recur and result in epilepsy.
Learn More:
What Is Epilepsy?Early Seizures
What is known about early seizures in TBI include:
- Approximately 1 in 10 people (10%) will experience an early seizure after TBI
- 50% of early seizures occur during the first 24 hours following TBI
- 25% of early seizures occur during the first hour following TBI
- Most very early seizures (within 24 hours of injury) are generalized tonic clonic seizures
- About 1 in 10 people will develop status epilepticus in the early period after a TBI
- Younger children are at highest risk for early post traumatic seizures and status epilepticus
- People who have head injuries that are more serious (examples: car accidents, fall from height, military blast injury), cause brain swelling or blood on the outside of the brain (subdural hemorrhage), or involve the brain being penetrated by a foreign object (example: bullet, combat injuries), or are accompanied by an extended period with loss of consciousness (>30 minutes) are more likely to have early seizures. One in four people who suffer from bleeding in the brain (intracerebral hematoma) requiring surgery or a skull fracture that compresses or injures brain tissue
- In some cases, even if a head injury is “mild” and a person has no evidence of injury to the brain on brain imaging with CT or MRI, a seizure may still occur
- EEG changes may or may not be present in the immediate period after a head injury
- If markers of seizures on EEG early after TBI this may mean a person is more likely to develop epilepsy
- People with early seizures after a brain trauma are at higher risk for developing post-traumatic epilepsy
Late Seizures
Seizures which occur more than a week after a traumatic brain injury are considered late seizures. Most often when this happens, it is because there has been more serious injury to brain cells and the chemical environment around the cells has also changed. Late seizures are more likely to lead to the complication of post-traumatic epilepsy.
What part of the brain is more at risk for injury and seizures?
When there is a traumatic blow to the head, or a jarring or shaking of the brain, the impact of the brain against the rough edges on the inside of the skull can cause tearing of the coverings of the brain, tissues, and blood vessels that may cause bleeding. The impact can also cause bruising (contusion) and swelling (edema) of the brain. Since the brain is covered by the skull, there is only a small amount of room for it to swell. This causes pressure inside the skull to increase, which can lead to additional widespread brain injury.
The brain does have some areas, which when injured, are more likely to result in recurrent seizures. This is partly due to their susceptibility for injury (areas that lie close to bony prominences of the skull) and an individual brain area’s propensity for seizures. Areas of the brain which are frequently involved include the temporal lobe, and the frontal and occipital lobes.
What changes in the brain can cause seizures after a TBI?
The structural, chemical and functional changes that result in seizures after TBI are still being studied. It is known that the type of changes that occur in brain tissue after a TBI depend on the type of trauma.
- Closed head injury can result in bleeding in the brain (hemorrhage), bruising of brain (contusions), shearing injury to the white matter tracts in the brain (diffuse axonal injury), brain swelling (edema) and a lack of blood flow to brain tissue (ischemia)
- Chemical changes in the brain which influence how brain cells function also known to occur after a TBI
- Penetrating injuries can result in a scar forming in brain tissue, or cause a scar to form that involves the outer layer of the brain (cortex) and its coverings (meninges)
- Electrophysiologic and imaging biomarkers are being studied as potential tools to better understand the brain changes related to seizures after TBI
- Blood and cerebrospinal fluid (CSF) biomarkers being studied may also make it possible to better understand the changes that occur leading to post-traumatic epilepsy
How are seizures treated in TBI?
Antiseizure medication (ASM) is first line therapy used to treat seizures after TBI.
- Treatment with ASM is typical if a person experiences even a single seizure early after TBI. Early treatment with ASM is started to help lower the likelihood of progression to status epilepticus
- Controlling seizures quickly is important to lower risk for further injury to the brain
- The length of treatment (weeks, months) with antiseizure medication is weighed carefully for each individual depending on extent of injury and likelihood for recurrent seizures
- In late seizures, there is a high, about 8 out of 10 people, recurrence rate for seizures
- Because of the high rate for repeat seizures, long term anticonvulsant treatment is recommended for people who have even one late (more than one week after TBI) seizure
- The choice of antiseizure medication will be based on the type of seizures a person has, and their individual medical history (co-morbid illness, medication tolerance)
Learn More:
List of Seizure MedicationsWhat is the outlook for people who have seizures after TBI?
- Between 25 and 40% of people will have remission (no seizure symptoms) of their epilepsy with initial treatment
- People who have frequent seizures in the first year after a TBI are less likely to have seizure remission and some of these people will have seizures that are resistant to medication
- People with moderate to severe TBI typically receive physical and cognitive rehabilitation that is individualized to their needs (physical therapy, occupational therapy, speech therapy, cognitive behavioral therapy)
- Psychology and psychiatry evaluation and treatment may be required for some people
- Social and community supports are very important for people living with physical, cognitive and psychological challenges as a result of traumatic brain injury
Resources:
National Brain Injury Information Center (NBIIC) at 800-444-6443
Post-Traumatic Epilepsy (PTE)
A person with post-traumatic epilepsy (PTE) is someone with risk for recurrent seizures as a result of a brain injury. About 1 in 50 people who have traumatic brain injuries will go on to develop PTE. There is a spectrum of severity of PTE that ranges from well controlled seizures to disabling seizures that are resistant to treatment.
What types of seizures do people with PTE have?
Most seizures (8 out of 10 people) in post-traumatic epilepsy are focal and may spread to become bilateral tonic clonic seizures. This means that they start in one area of the brain (focal) but spread to involve the entire brain (generalized). Sometimes the beginning of these seizures (focal onset) can be determined and relates to the area of the brain injured, other times it is harder to determine where a seizure begins. A person may have focal aware or focal impaired awareness seizures but these are less frequent (occur in about 2 out of 10 people).

In 1 out of 2 people post traumatic epilepsy occurs within one year of their brain injury. The more severe the head injury the longer a person is at risk for developing epilepsy. Risk for PTE developing decreases substantially with time but can extend out to 15 years after the original traumatic injury for people with the most severe brain injuries.
A person is at higher risk for developing PTE if:
- They experience early seizures after the TBI
- They had bleeding into brain tissue or bruising (contusion) of the brain at time of injury
- They suffered a skull fracture and a piece of the skull shifted into the brain injuring brain tissue, or compressed the brain (depressed skull fracture)
- A penetrating brain trauma occurred (example bullet, combat injury)
- They have a head injury that has occurred in relation to alcohol use
- Surgery needed to remove bleeding (hematoma) from the brain, remove a foreign object from the brain, or to drain fluid (ventriculostomy) from the brain if there is swelling in the brain related to the trauma
- EEG has abnormalities which appear early in the course post injury
- A person is older than age 65
- A person has a family history of epilepsy

Is surgical treatment an option for PTE?
Surgery may be an option for people with drug resistant post-traumatic epilepsy (i.e. those who continue to have seizures despite trials of two more more ASMs.) Similar to other types of epilepsy, the goal of surgery in post-traumatic epilepsy is to safely remove epileptogenic brain tissue.
A pre-surgical evaluation will take place to determine where seizures are coming from and to decide if a person is a surgical candidate.
Vagus nerve stimulation should be considered for people who have medication resistant epilepsy and are not candidates for surgical resection. Newer surgical therapies, responsive neurostimulation (RNS) and deep brain stimulation are two techniques available to treat medication resistant seizures in epilepsy which may provide possibilities for further treatment in PTE .
Comorbidities in PTE
Comorbidities are medical conditions that occur at the same time which can influence a person’s health. Comorbidities in PTE can include physical, cognitive and psychiatric disorders. The evaluation and treatment of PTE needs careful consideration of the possible co-morbid disease, the way the comorbid diseases is being treated and how these factors might influence seizures or the treatments used to control seizures in PTE.
Health problems that may occur alongside PTE include:
- Physical- Decreased mobility, poor coordination, headache, chronic pain, sleep or movement disorders
- Cognitive- Problems with memory or attention, poor decision making, speech problems, impulsivity, difficulty learning
- Psychiatric- Anxiety, depression, personality changes, aggressive behavior, PTSD, suicide, PNES
Resources
Epilepsy Centers
Epilepsy centers provide you with a team of specialists to help you diagnose your epilepsy and explore treatment options.
Epilepsy Medication
Find in-depth information on anti-seizure medications so you know what to ask your doctor.
Epilepsy and Seizures Helpline
Call our Epilepsy and Seizures Helpline and talk with an epilepsy information specialist or submit a question online.
Tools & Resources
Get information, tips, and more to help you manage your epilepsy.
Related Stories

Press Releases
Epilepsy Community Celebrates Senate Passage of the National Plan for Epilepsy Act
Read Story
Press Releases
New Joint Statement Highlights Seizure Detection Devices as Tool for Safety in Epilepsy Care
Read Story