
Temporal Lobe Epilepsy (TLE)
Medial TLE can be associated with hippocampal sclerosis, as shown on the MRI scan above.
What is temporal lobe epilepsy (TLE)?
Temporal lobe epilepsy is the most common form of focal epilepsy. About 6 out of 10 people with focal epilepsy have temporal lobe epilepsy. Seizures in TLE start or involve in one or both temporal lobes in the brain.
There are two types of TLE:
- Mesial temporal lobe epilepsy (MTLE) involves the middle or internal structures of the temporal lobe. Seizures often begin in a structure of the brain called the hippocampus or in the nearby surrounding area. MTLE accounts for almost 80% of all temporal lobe seizures.
- Neocortical or lateral temporal lobe epilepsy involves the outer part of the temporal lobe.
Mesial temporal lobe epilepsy usually begins around ages 10 - 20, but it can start at any age. Sometimes, a person has had a prolonged seizure with high fever or another type of injury to the brain in their early years which may have damaged the mesial temporal lobe of the brain.
There are a lot of older names for seizures that occur in TLE, including "psychomotor seizures," "limbic seizures," "temporal lobe seizures," "complex partial," and "simple partial." The modern name for these seizures is "focal onset seizures." Focal seizures are then described by whether a person stays awake and conscious or has impaired consciousness during a seizure.
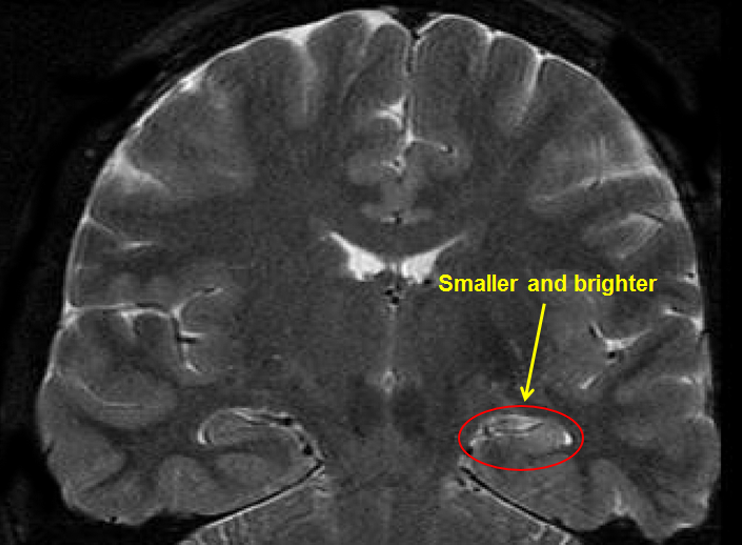
Mesial temporal lobe epilepsy is often associated with changes or abnormal findings on MRI (magnetic resonance imaging). One of the most common findings is scarring in the temporal lobe. This is called hippocampal sclerosis (sclerosis means hardening or scarring). It may look like the hippocampus on one side, or both, has shrunk or is smaller. (*MRI provides a mirror image of the brain, so the right and left sides of the brain are reversed in the image.)
Right Mesial Temporal Sclerosis (MTS)
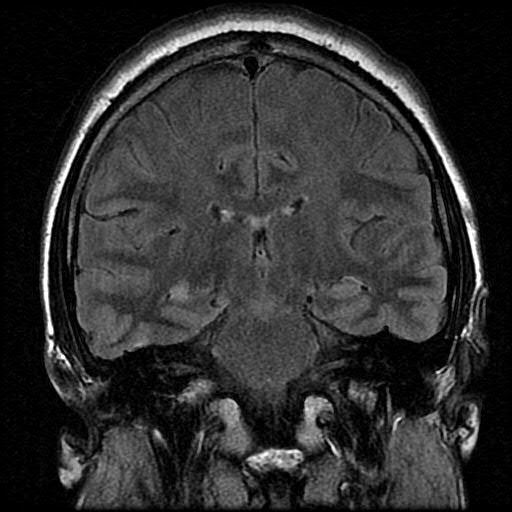
Right Mesial Temporal Sclerosis (MTS) with Flair
When looking at an MRI the right and left sides of the brain are reversed in the image. Also, see arrow in figure at the top of the page.
Common risk factors that lead to developing TLE include:
- Brain injury including head trauma with loss of consciousness, birth injury, infections such as encephalitis or meningitis that happen early in life
- Changes in the structure of a temporal lobe, such as brain malformations or tumors
- The most common risk factor is a prolonged febrile seizure.
- About 2 out of 3 people with TLE have had a history of febrile seizures.
- Three out of 4 of these were either prolonged or had complex features.
- It is important to know that the vast majority of people with febrile seizures do not develop temporal lobe epilepsy.
Learn More:
Contact Our HelplineWhat type of seizures are seen?
Seizures in TLE include focal conscious seizures, such as auras, and focal impaired consciousness seizures.
- Auras are the same as focal seizures with preserved consciousness. They used to be called simple partial seizures. They are the first symptoms of a seizure.
- The most common auras are feelings of déjà-vu or some stomach upset.
- Feelings of fear, panic, anxiety, a rising sensation coming from the stomach to the chest or throat, or butterflies with nausea are other common auras.
- Some people may sense an unusual smell. This symptom may raise the possibility of a lesion or tumor in the hippocampus of the temporal lobe.
- Sometimes the auras can be very hard to describe.
Focal seizures with impaired consciousness used to be called complex partial seizures.
- During this type of seizure, a person may have a fixed stare, be unaware or confused about what is going on around them, have fumbling with their fingers, or lip-smacking movements. The seizures usually last 30 seconds to a couple of minutes.
- There can be unusual posturing (movement or positioning) in an arm. The precise movements made can help neurologists identify where seizures start in the brain.
- Some people also speak gibberish or lose their ability to speak in a sensible manner. Language problems are more common if the seizures are coming from the temporal lobe of the brain on the same side that controls language (sometimes called the dominant side).
- Seizures in neocortical or lateral temporal lobe epilepsy often start with an auditory aura, such as buzzing or hearing a specific sound.
- The focal seizure can spread into generalized tonic-clonic jerking. The person may be weak after the seizure has stopped.
- Somet people can also have prolonged seizures (lasting 5 minutes or more) or repeated seizures without returning to consciousness in between. When this happens, the condition is called status epilepticus and is a seizure emergency for which medical help should be called.
A Typical Story
"I get the strangest feeling – most of it can`t be put into words."
"The whole world suddenly seems more real at first. It's as though everything becomes crystal clear. Then I feel as if I'm here but not here, kind of like being in a dream. It's as if I've lived through this exact moment many times before. I hear what people say, but they don't make sense. I know not to talk during the episode, since I just say foolish things. Sometimes I think I'm talking but later people tell me that I didn't say anything. The whole thing lasts a minute or two."
How is TLE diagnosed?
Mesial temporal lobe epilepsy is a clinical diagnosis. This means that a number of factors are put together. There isn’t one test for TLE.
- It’s important to listen to a person describe their seizures in as much detail as possible or by hearing observations of a witness.
- An MRI of the brain should be done to look for changes in the temporal lobe.
- An EEG (electroencephalogram) should be done and often shows spike or sharp waves in the tip or front of the temporal lobe. These can be seen when a person is awake or asleep.
- When seizures arise in more mesial (middle) temporal lobe areas, the EEG may only show rhythmic slowing during seizures. These may be hard to diagnose unless a typical seizure is recorded on the EEG.
Download these forms to help record and describe seizures:
How is TLE treated?
Talking with your healthcare team about your seizure control and how seizures affect your life is the first step in finding the best treatment plan. Consider seeing a neurologist who specializes in epilepsy (called an epileptologist) and have an evaluation at an epilepsy center to explore all treatment options, including surgery, devices, and dietary therapy. There may also be ongoing clinical trials looking at new treatment options.
Anyone with TLE who has had breakthrough seizures after trying 2 or more antiseizure drugs should be seen by an epileptologist at an epilepsy surgery center as early as possible. The sooner a person is seen for surgical evaluation, the greater chance of success from surgery.
Medication
Many people with temporal lobe epilepsy achieve full seizure control with anti-seizure medicines. But almost a third of people may not respond to medictherapy.
Uncontrolled seizures may cause a number of problems. For example, people often report problems with memory, socialization, and a fear of leaving their home. They may restrict their daily activities, which leads to a decrease in quality of life.
Other Treatments
If seizures fail to respond to medication, then epilepsy surgery may be an option. When an MRI shows hippocampal sclerosis in the side of the brain that is not involved with language and EEGs show seizures starting in that same area, seizures may be cured by surgery. In some cases, up to 7 out of 10 people with Mcan be seizure-free after surgery with few problems afterwards.
Neuropsychological testing is important for any person considering epilepsy surgery. Testing helps guide doctors, people with epilepsy, and families about possible cognitive risks (attention, memory, and learning) compared to benefits of seizure control.
If surgery is not possible or doesn't work, devices such as vagus nerve stimulation (VNS), responsive neurostimulation (RNS) or deep brain stimulation (DBS) may help.
What is the outlook?
Two out of 3 people with temporal lobe epilepsy achieve good seizure control with seizure medication. Seizures may also go away in some children with TLE. A good outcome is most often seen in people with normal MRI scans.
If the MRI is abnormal, there is a much higher risk that seizures will not respond to medicines (called drug-resistant epilepsy or DRE). Overall, the prognosis for people with drug-resistant medial temporal lobe epilepsy includes a higher risk for memory and mood problems, lower quality of life, and an increased risk for sudden unexpected death in epilepsy (SUDEP). People with DRE should seek out an epilepsy center to be evaluated and to consider advanced treatments like neuromodulatory devices, epilepsy surgery, ketogenic diets, or clinical trials of new therapies.
Learn More:
Donate to Support Our MissionResources
Epilepsy Centers
Epilepsy centers provide you with a team of specialists to help you diagnose your epilepsy and explore treatment options.
Epilepsy Medication
Find in-depth information on anti-seizure medications so you know what to ask your doctor.
Epilepsy and Seizures Helpline
Call our Epilepsy and Seizures Helpline and talk with an epilepsy information specialist or submit a question online.
Tools & Resources
Get information, tips, and more to help you manage your epilepsy.
Related Stories


Press Releases
New Joint Statement Highlights Seizure Detection Devices as Tool for Safety in Epilepsy Care
Read Story Press Releases
Epilepsy Foundation of America Awards $250,000 at 14th Annual Shark Tank Competition
Read Story